
 Cardiovascular Physiology Concepts, 3rd edition textbook, Published by Wolters Kluwer (2021)
Cardiovascular Physiology Concepts, 3rd edition textbook, Published by Wolters Kluwer (2021) Normal and Abnormal Blood Pressure, published by Richard E. Klabunde (2013)
Normal and Abnormal Blood Pressure, published by Richard E. Klabunde (2013)Cardiac Action Potentials
Non-nodal Cell Action Potentials
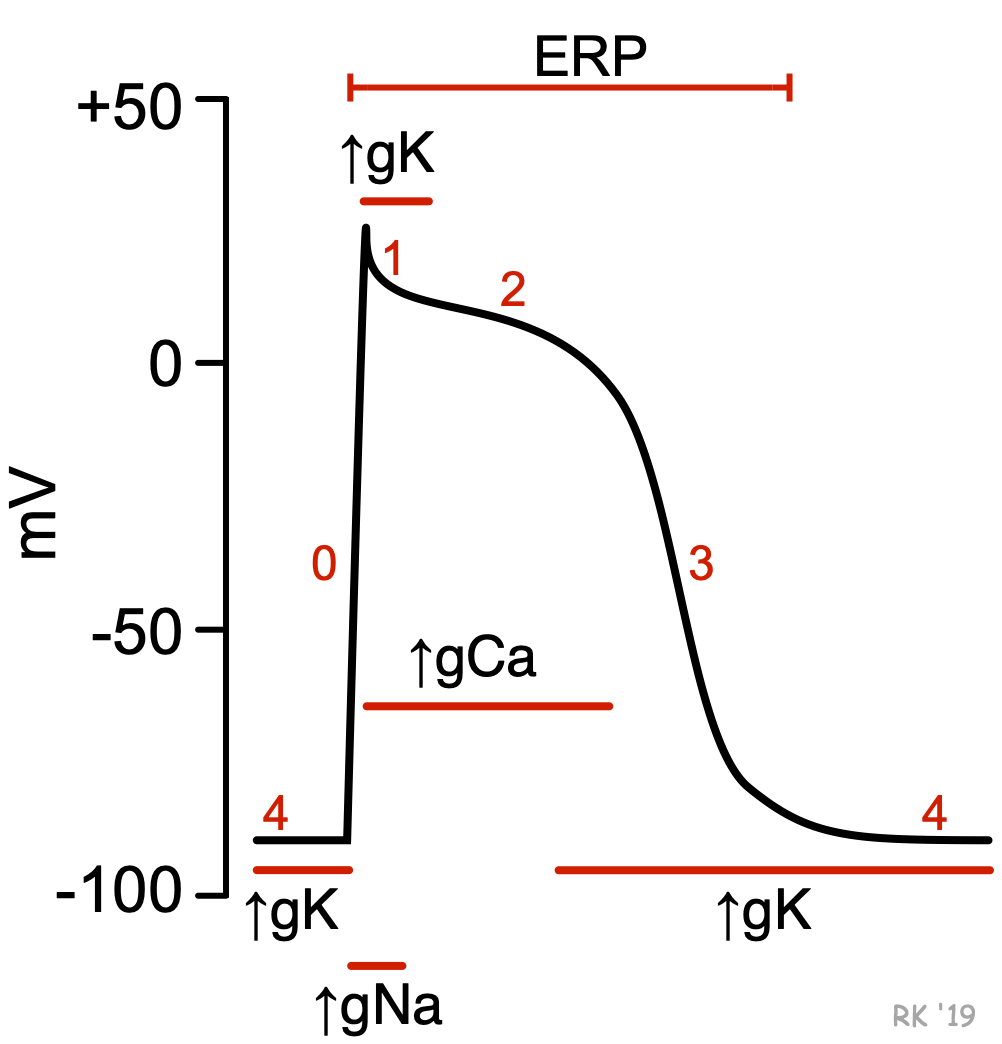 Non-nodal action potentials, sometimes referred to as "fast response" action potentials, are characteristic of atrial and ventricular myocytes, and the fast-conducting Purkinje system in the ventricles. These action potentials are distinguished from slow response action potentials by having a true resting potential (phase 4), a fast depolarization phase (phase 0), and a prolonged plateau phase (phase 2) as shown in the figure. Because action potentials are determined by the movement of different ions (ion currents) into and out of the cell, changes in membrane conductance (g) to these ions alter the membrane potential to produce the action potentials.
Non-nodal action potentials, sometimes referred to as "fast response" action potentials, are characteristic of atrial and ventricular myocytes, and the fast-conducting Purkinje system in the ventricles. These action potentials are distinguished from slow response action potentials by having a true resting potential (phase 4), a fast depolarization phase (phase 0), and a prolonged plateau phase (phase 2) as shown in the figure. Because action potentials are determined by the movement of different ions (ion currents) into and out of the cell, changes in membrane conductance (g) to these ions alter the membrane potential to produce the action potentials.
Action potential phases:
- Phase 0: Rapid depolarization
- ↑ Na+ and ↓ K+ conductance - Phase 1: Initial repolarization
- ↓ Na+ and ↑ K+ conductance - Phase 2: Plateau phase
- ↑ Ca++ conductance - Phase 3: Repolarization
- ↑ K+ and ↓ Ca++ conductance - Phase 4: Resting potential
- ↑ K+ and ↓ Na+ and ↓ Ca++ conductance
For more detailed information, click here.
Antiarrhythmic drugs that block or facilitate the movement of these ions are used to alter cardiac action potentials to prevent or stop arrhythmias. In non-nodal tissue, sodium-channel blockers decrease the fast inward movement of Na+, which decreases the slope of phase 0 and the magnitude of depolarization. The principal effect of this change is a reduction in conduction velocity. These drugs also increase the effective refractory period (ERP) by delaying the reactivation of fast-sodium channels. Potassium-channel blockers delay the onset and prolong phase 3 repolarization, which lengthens the action potential duration and ERP.
Nodal Cell Action Potentials
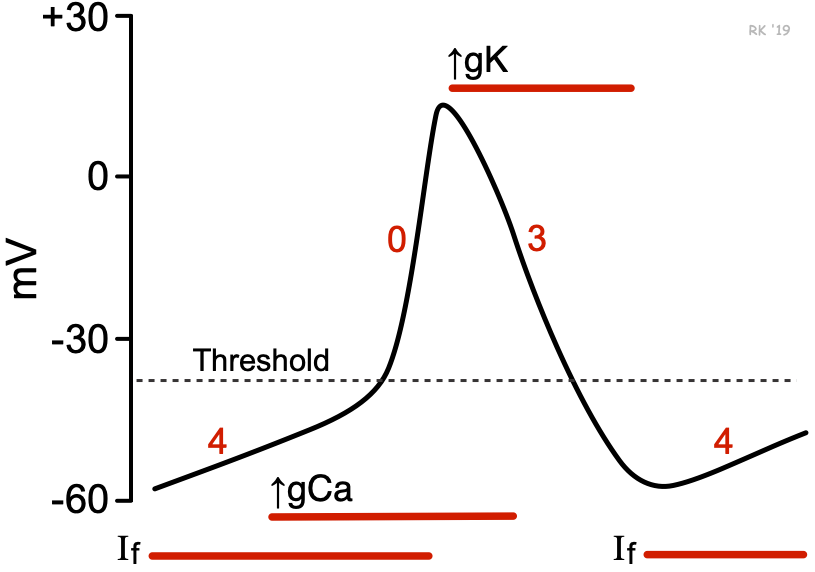 Nodal action potentials, sometimes referred to as "slow response" action potentials, are characteristic of action potentials found in the sinoatrial node and atrioventricular (AV) node. These action potentials display automaticity, or pacemaker activity, and therefore undergo spontaneous depolarization. Their depolarization phase is less rapid, and they have a shorter action potential duration than non-nodal, fast response action potentials. Furthermore, they have no phase 1 or phase 2.
Nodal action potentials, sometimes referred to as "slow response" action potentials, are characteristic of action potentials found in the sinoatrial node and atrioventricular (AV) node. These action potentials display automaticity, or pacemaker activity, and therefore undergo spontaneous depolarization. Their depolarization phase is less rapid, and they have a shorter action potential duration than non-nodal, fast response action potentials. Furthermore, they have no phase 1 or phase 2.
Action potential phases:
- Phase 0: Depolarization
- ↑ Ca++ and ↓ K+ conductance - Phase 3: Repolarization
- ↑ K+ and ↓ Ca++ conductance - Phase 4: Spontaneous depolarization
- "Funny" currents (If) through slow inward Na+ channels
- ↑ Ca++ and ↓ K+ conductance
For more detailed information, click here.
Changes in the membrane conductance to calcium and potassium ions alter slow-response action potentials. Calcium-channel blockers reduce the slope of phase 4, decreasing the rate of spontaneous depolarization, which reduces the rate of pacemaker firing. These drugs also decrease the slope of phase 0, which slows conduction velocity within the AV node. The AV nodal ERP is also lengthened by calcium-channel blockers. Potassium-channel blockers delay phase 3 repolarization, lengthening the action potential duration and ERP.
Revised 11/30/2023